|
|
||
|
||
|
Privacy Policy | Editorial Policy | Profit Policy | Join the Association | List of Members | Contact us | Index | Links |
||
|
Back Go to page: 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Forward
|
||
|
Health and Life Style. |
||
| Veterans and Veterans Families Counselling Service (VVCS) can be reached 24 hours a day across Australia for crisis support and free and confidential counseling. Phone 1800 011 046. VVCS is a service founded by Vietnam Veterans. |
||
|
Contents:
Why does time move faster as we age.
|
||
|
Why time really does move faster as we get older.
Old codgers everywhere are saying this right now: “We’re half way through the year already? Geez, the years go by faster and faster”. Well they seem to and for years researchers have been trying to figure out why time seems to fly as we age. |
||
|
|
||
|
According to an intriguing new theory, published recently, the “apparent temporal discrepancy” can be blamed on the ever-slowing speed at which images are collected, or perceived in the surrounding environment and processed by the ageing human brain.
In short, we don’t see as much as we used to.
The study author explains it this way.
As tangled webs of nerves and neurons mature, they grow in size and complexity, leading to longer paths for signals to traverse. As those paths then begin to age, they also degrade, giving more resistance to the flow of electrical signals. These phenomena cause the rate at which new mental images are acquired and processed to decrease with age. This is evidenced by how often the eyes of infants move compared to adults, because infants process images faster than adults, their eyes move more often, acquiring and integrating more information.
A slower view of the world speeds time up.
The end result is that, because older people are viewing fewer new images in the same amount of actual time, it seems to them as though time is passing more quickly. The human mind senses time changing when the perceived images change. The present is different from the past because the mental viewing has changed, not because somebody’s clock rings. Days seemed to last longer in your youth because the young mind receives more images during one day than the same mind in old age.
The mechanism central to this theory is what’s known as “saccades frequency”.
Saccadic eye movements are unconscious, unfocused jerks during which the eye isn’t focused on anything; they occur a few times a second. In between this flickering, our eyes fixate on something and the brain processes what’s being perceived. There’s a cat on the TV that is playing in the background, for example. In human infants, those fixation periods are shorter than in adults and the net result is babies actually see more, and their brains are busier, in the same amount of time. When you are young and your brain is busy taking in new things, time seems to be pass more slowly. As you get older, the rate at which we flick from one thing to the other slows down, giving the sense that time passes more rapidly. It’s the release of the neurotransmitter dopamine that helps us learn to measure time.
Beyond the age of 20 and continuing into old age, dopamine levels drop, making time appear to run faster. In 1996, in a variation of a common experiment exploring time perception, a psychologist in the US asked 25 people aged between 19 and 24, and 15 older people aged between 60 and 80, to estimate a three-minute interval by counting seconds. They were told to use the “1, 1000, 2, 1000” technique. The youngsters averaged three minutes and three seconds. For the oldies, all of them still busy people, engaged with life, an average of three minutes and 40 seconds skipped by before they thought three minutes had elapsed. The psychologist speculated that the brain’s internal clock, a theoretical idea of a clock that tracks time intervals, and separate from the circadian clock that controls sleep and wake cycles, runs more slowly as we age. Dopamine being the villain here.
As people age, brain cells that produce dopamine begin to deteriorate in the basal ganglia and substantia nigra. It’s these regions that contain the workings of this internal clock.
|
||
|
Why is it the one who snores the loudest is always the first to fall asleep.
|
||
|
Huntington's disease is an inherited disease that causes the progressive breakdown (degeneration) of nerve cells in the brain. Huntington's disease has a broad impact on a person's functional abilities and usually results in movement, thinking (cognitive) and psychiatric disorders. Most people with Huntington's disease develop signs and symptoms in their 30s or 40s. But the disease may emerge earlier or later in life.
When the disease develops before age 20, the condition is called juvenile Huntington's disease. An earlier emergence of the disease often results in a somewhat different set of symptoms and faster disease progression. Medications are available to help manage the symptoms of Huntington's disease, but treatments can't prevent the physical, mental and behavioural decline associated with the condition.
Huntington's disease usually causes movement, cognitive and psychiatric disorders with a wide spectrum of signs and symptoms. Which symptoms appear first varies greatly among affected people. During the course of the disease, some disorders appear to be more dominant or have a greater effect on functional ability.
The movement disorders associated with Huntington's disease can include both involuntary movement problems and impairments in voluntary movements, such as:
Impairments in voluntary movements, rather than the involuntary movements, may have a greater impact on a person's ability to work, perform daily activities, communicate and remain independent.
Cognitive impairments often associated with Huntington's disease include:
The most common psychiatric disorder associated with Huntington's disease is depression. This isn't simply a reaction to receiving a diagnosis of Huntington's disease, instead, depression appears to occur because of injury to the brain and subsequent changes in brain function. Signs and symptoms may include:
Other common psychiatric disorders include:
In addition to the above symptoms, weight loss is common in people with Huntington's disease, especially as the disease progresses.
The start and progression of Huntington's disease in younger people may be slightly different from that in adults. Problems that often present themselves early in the course of the disease include:
See your doctor if you notice changes in your movements, emotional state or mental ability. The signs and symptoms of Huntington's disease can be caused by a number of different conditions. Therefore, it's important to get a prompt, thorough diagnosis.
Cause.
Huntington's disease is caused by an inherited defect in a single gene. Huntington's disease is an autosomal dominant disorder, which means that a person needs only one copy of the defective gene to develop the disorder. With the exception of genes on the sex chromosomes, a person inherits two copies of every gene, one copy from each parent. A parent with a defective gene could pass along the defective copy of the gene or the healthy copy. Each child in the family, therefore, has a 50 percent chance of inheriting the gene that causes the genetic disorder.
After the start of Huntington's disease, a person's functional abilities gradually worsen over time. The rate of disease progression and duration varies. The time from disease emergence to death is often about 10 to 30 years. Juvenile Huntington's disease usually results in death within 10 years after symptoms develop. The clinical depression associated with Huntington's disease may increase the risk of suicide. Some research suggests that the greater risk of suicide occurs before a diagnosis is made and in the middle stages of the disease when a person has begun to lose independence.
Eventually, a person with Huntington's disease requires help with all activities of daily living and care. Late in the disease, he or she will likely be confined to a bed and unable to speak, however, he or she is generally able to understand language and has an awareness of family and friends. Common causes of death include:
People with a known family history of Huntington's disease are understandably concerned about whether they may pass the Huntington gene on to their children. These people may consider genetic testing and family planning options.
If an at-risk parent is considering genetic testing, it can be helpful to meet with a genetic counsellor. A genetic counsellor will discuss the potential risks of a positive test result, which would indicate the parent will develop the disease. Also, couples will need to make additional choices about whether to have children or to consider alternatives, such as prenatal testing for the gene or in vitro fertilization with donor sperm or eggs.
Another option for couples is in vitro fertilization and preimplantation genetic diagnosis. In this process, eggs are removed from the ovaries and fertilized with the father's sperm in a laboratory. The embryos are tested for presence of the Huntington gene, and only those testing negative for the Huntington gene are implanted in the mother's uterus.
|
||
|
Wife: "The car is not starting. Dashboard shows the sign of a person sitting on a toilet". Husband: "What? Send me a picture." |
||
|
Giving up smoking can be one of the hardest things you’ll ever do. Some people are lucky, they can just toss the pack in the bin and that’s it, others will give up many many times each time their smoke free period would last sometimes not even one day. Others will give up for several weeks until they are with a group and see someone else light up then the urge is too great and they just start up again. Others will give up and stay off the durries until they do something that they always associated with having a smoke – like having a drink with the boys/girls. And there are those who can’t give up no matter what they try.
Once hooked on the things it is very hard to unhook oneself – but why is that?
The Mayo Clinic has produced a little video explaining why, it is very interesting. Click the pic below to see it. |
||
|
|
||
|
Just before the funeral services, the undertaker came up to the very elderly widow and asked, "How old was your husband?" "98," she replied: "Two years older than me" "So you're 96," the undertaker commented. She responded, "Hardly worth going home, is it?"
|
||
|
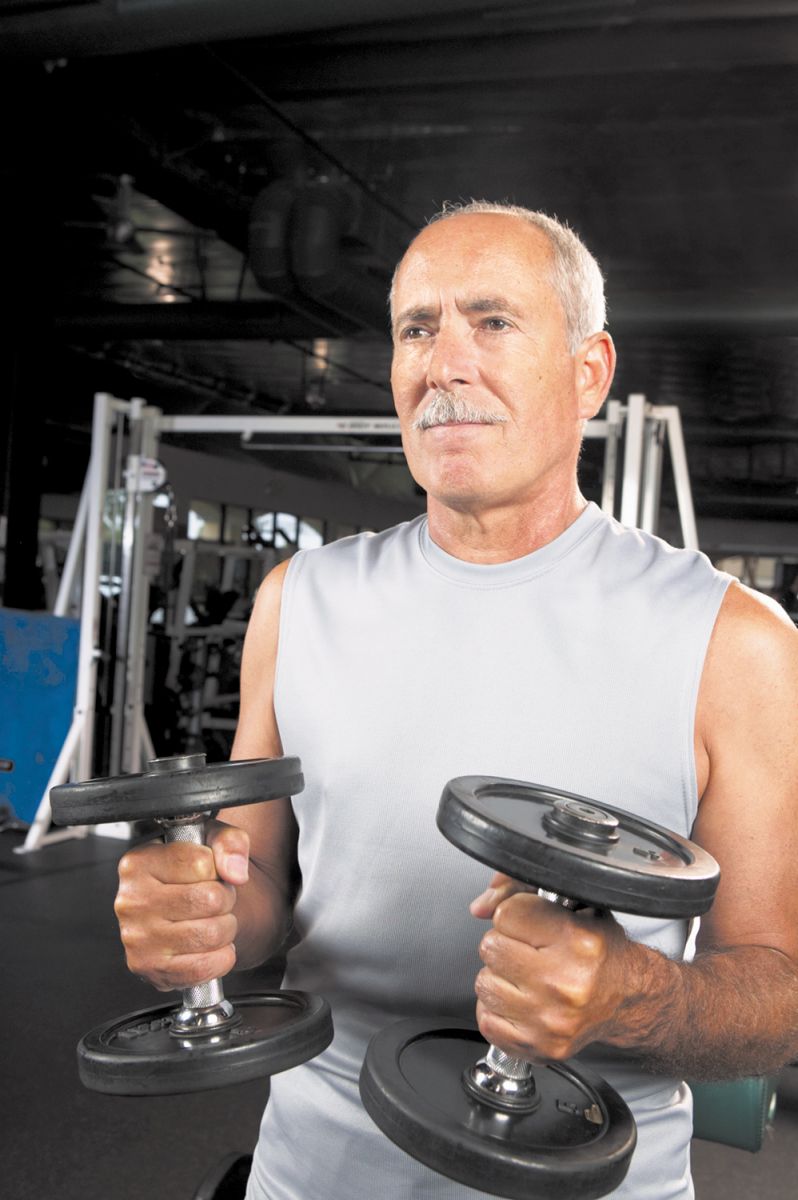
The saying goes there are two certainties in life: death and taxes. But men should also add loss of muscle mass to the list.
Age-related muscle loss, called sarcopenia, is a natural part of aging. After age 30, we begin to lose as much as 3% to 5% per decade. Most men will lose about 30% of their muscle mass during their lifetimes. Less muscle means greater weakness and less mobility, both of which may increase your risk of falls and fractures.
But just because you lose muscle mass does not mean it is gone forever. Older men can indeed increase muscle mass lost as a consequence of aging, it takes work, dedication and a plan, but it is never too late to rebuild muscle and maintain it.
One possible contributor to sarcopenia is the natural decline of testosterone, the hormone that stimulates protein synthesis and muscle growth. Think of testosterone as the fuel for your muscle-building fire. Some research has shown that supplemental testosterone can add lean body mass, that is, muscle, in older men, but there can also be adverse effects. The best means to build muscle mass, no matter your age, is progressive resistance training (PRT). With PRT, you gradually amp up your workout volume, weight, reps, and sets as your strength and endurance improves.
This constant challenging builds muscle and keeps you away from plateaus where you stop making gains.
Your diet also plays a role in building muscle mass. Protein is the king of muscle food. The body breaks it down into amino acids which it uses to build muscle, however, older men often experience a phenomenon called anabolic resistance, which lowers their bodies' ability to break down and synthesize protein. Therefore, as with PRT, if you are older, you need more. A recent study in the journal Nutrients suggests a daily intake of 1 to 1.3 grams (g) of protein per kilogram of body weight for older adults who do resistance training. For example, an 80kg man would need about 80g to 103g of protein a day (1 egg gives you about 15g of protein). If possible, divide your protein equally among your daily meals to maximize muscle protein synthesis.
This is a high amount compared with the average diet, but there are many ways to get the extra protein you need. Animal sources (meat, eggs, and milk) are considered the best, as they provide the proper ratios of all the essential amino acids, yet, you want to stay away from red and processed meat because of high levels of saturated fat and additives. Instead, opt for healthier choices, such as:
Protein powders can offer about 30g per scoop and can be added to all kinds of meals like oatmeal, shakes, and yogurt. While food sources are the best, supplemental protein can help if you struggle with consuming enough calories and protein from your regular diet.
Building muscle is not all about strength, you also need power. Muscle power, how fast and efficiently you move, is more connected to the activities of daily living and physical function than muscular strength. A good way to improve overall muscle power is with your legs, since they are most responsible for mobility. Doing quicker movements against resistance, like one's own body weight, can be an effective means of developing power. For instance, when rising from a seated position, try to do it quickly. When climbing stairs, hold the handrail and push off a step as fast as possible. It does not have to be every step, begin with one to three steps, but this teaches your muscles to use strength in a more effective way.
To gain more muscle mass, older men need a structured and detailed PRT program which should be tailored to the individual with the goals being progression and improvement. It should focus on individual elements like specific exercises, load, repetitions, and rest periods, and should challenge but not overwhelm.
A typical training program might include:
After you have established a routine, there are several ways to progress. The easiest is to add a second and then a third set of the exercises. Another way is to decrease the number of reps per set and increase the weight or resistance to the point where you are able to complete at least eight reps, but no more than 12. As you improve, you can increase weight by trial and error, so you stay within the range of eight to 12 reps.
What's better for strength training — one set or multiple sets?
For most people, a single set of 12 to 15 repetitions with the proper weight can build strength and improve fitness as effectively as can multiple sets of the same exercise.
The one-set approach also has the advantage of saving time, which makes it easier to fit into an exercise routine. During strength training, simply choose a weight that tires your muscles around the 12th to 15th repetition. As this becomes easier, gradually increase the amount of weight to maintain a 12- to 15-repetition fatigue. It's important to use proper technique to avoid injury. Also, take time to rest between each exercise to give your muscles time to recover.
Although a single set of strength training exercises can improve muscle strength and fitness, the number of sets that you perform may differ depending on your fitness goals.
|
||
|
|
||
|
|
||
|
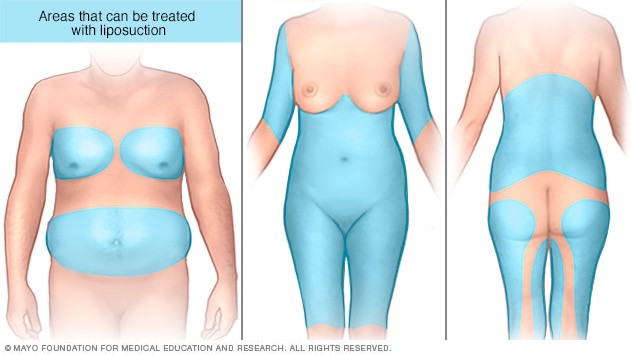
Liposuction is a surgical procedure that uses a suction technique to remove fat from specific areas of the body, such as the abdomen, hips, thighs, buttocks and arms or neck. Liposuction also shapes (contours) these areas. Other names for liposuction include lipoplasty and body contouring.
Liposuction isn't typically considered an overall weight-loss method or a weight-loss alternative. If you're overweight, you're likely to lose more weight through diet and exercise or through bariatric procedures, such as gastric bypass surgery, than you would with liposuction. You may be a candidate for liposuction if you have too much body fat in specific spots but otherwise have a stable body weight.
It is used to remove fat from areas of the body that haven't responded to diet and exercise, such as the:
In addition, liposuction can sometimes be used for breast reduction or treatment of gynecomastia (Enlarged Breast Tissue in Men). When you gain weight, fat cells increase in size and volume. In turn, liposuction reduces the number of fat cells in a specific area. The amount of fat removed depends on the appearance of the area and the volume of fat. The resulting contour changes are generally permanent — as long as your weight remains stable.
After liposuction, the skin moulds itself to the new contours of the treated areas. If you have good skin tone and elasticity, the skin is likely to appear smooth. If your skin is thin with poor elasticity, however, the skin in the treated areas may appear loose. Liposuction doesn't improve cellulite dimpling or other skin surface irregularities. Likewise, liposuction doesn't remove stretch marks. To be a candidate for liposuction, you must be in good health without conditions that could complicate surgery, such as restricted blood flow, coronary artery disease, diabetes or a weak immune system.
As with any major surgery, liposuction carries risks, such as bleeding and a reaction to anaesthesia. Possible complications specific to liposuction include:
Contour irregularities. Your skin may appear bumpy, wavy or withered due to uneven fat removal, poor skin elasticity and unusual healing. These changes may be permanent. Damage beneath the skin from the thin tube (cannula) that's used during liposuction may give the skin a permanent spotted appearance. Fluid accumulation. Temporary pockets of fluid (seromas) can form under the skin. This fluid may need to be drained with a needle. Numbness. You may feel temporary or permanent numbness in the affected area. Temporary nerve irritation also is possible. Infection. Skin infections are rare but possible. A severe skin infection may be life-threatening. Internal puncture. Rarely, a cannula that penetrates too deeply may puncture an internal organ. This may require emergency surgical repair. Fat embolism. Pieces of loosened fat may break away and become trapped in a blood vessel and gather in the lungs or travel to the brain. A fat embolism is a medical emergency. Kidney and heart problems. Shifts in fluid levels as fluids are being injected and suctioned out can cause potentially life-threatening kidney, heart and lung problems. Lidocaine toxicity. Lidocaine is an anaesthetic often administered with fluids injected during liposuction to help manage pain. Although generally safe, in rare circumstances, lidocaine toxicity can occur, causing serious heart and central nervous system problems.
The risk of complications increases if the surgeon is working on larger surfaces of your body or doing multiple procedures during the same operation. Talk to your surgeon about how these risks apply to you.
Before the procedure, your surgeon will recommend that you stop taking certain medications, such as blood thinners or NSAIDs, at least three weeks prior to surgery. You may also need to get certain lab tests before your procedure. If your procedure requires the removal of only a small amount of fat, the surgery may be done in an office setting. If a large amount of fat will be removed, or if you plan to have other procedures done at the same time, the surgery may take place in a hospital followed by an overnight stay. In either case, arrange for someone to drive you home and stay with you for at least the first night after the procedure.
How your liposuction procedure is done depends on the specific technique that's used. Your surgeon will select the appropriate technique based on your treatment goals, the area of your body to be treated, and whether you have had other liposuction procedures in the past.
Tumescent liposuction. This is the most common type of liposuction. The surgeon injects a sterile solution, a mixture of salt and water, which aids fat removal, an anaesthetic (lidocaine) to relieve pain and a drug (epinephrine) that causes the blood vessels to constrict, into the area that's being treated. The fluid mixture causes the affected area to swell and stiffen. He/she then makes small cuts into your skin and inserts a thin tube called a cannula under your skin. The cannula is connected to a vacuum that suctions fat and fluids from your body. Your body fluid may be replenished through an intravenous (IV) line. Ultrasound-assisted liposuction (UAL). This type of liposuction is sometimes used in conjunction with traditional liposuction. During UAL, the surgeon inserts a metal rod that emits ultrasonic energy under your skin. This ruptures the fat-cell walls and breaks down the fat for easier removal. A new generation of UAL called VASER-assisted liposuction uses a device that may improve skin contouring and reduce the chance of skin injuries. Laser-assisted liposuction (LAL). This technique uses high-intensity laser light to break down fat for removal. During LAL, the surgeon inserts a laser fibre through a small incision in the skin and emulsifies fat deposits. The fat is then removed via a cannula. Power-assisted liposuction (PAL). This type of liposuction uses a cannula that moves in a rapid back-and-forth motion. This vibration allows the surgeon to pull out tough fat more easily and faster. PAL may sometimes cause less pain and swelling and can allow the surgeon to remove fat with more precision. Your surgeon may select this technique if large volumes of fat need to be removed or if you've had a previous liposuction procedure.
Some liposuction procedures may require only local or regional anaesthesia, anaesthesia limited to a specific area of your body. Other procedures may require general anaesthesia which induces a temporary state of unconsciousness. You may be given a sedative, typically through an IV injection, to help you remain calm and relaxed. The surgical team will monitor your heart rate, blood pressure and blood oxygen level throughout the procedure. If you are given local anaesthesia and feel pain during the procedure, tell your surgeon. The medication or motions may need adjustment.
The procedure may last up to several hours, depending on the extent of fat removal. If you've had general anaesthesia, you'll wake in a recovery room and typically spend at least a few hours in the hospital or clinic so that medical personnel can monitor your recovery. If you're in a hospital, you may stay overnight to make sure that you're not dehydrated or in shock from fluid loss.
Expect some pain, swelling and bruising after the procedure. Your surgeon may prescribe medication to help control the pain and antibiotics to reduce the risk of infection. After the procedure, the surgeon may leave your incisions open and place temporary drains to promote fluid drainage. You usually need to wear tight compression garments, which help reduce swelling, for a few weeks. You may also need to wait a few days before returning to work and a few weeks before resuming your normal activities, including exercise. During this time, expect some contour irregularities as the remaining fat settles into position.
After liposuction, swelling typically subsides within a few weeks. By this time, the treated area should look less bulky. Within several months, expect the treated area to have a leaner appearance. It's natural for skin to lose some firmness with aging, but liposuction results are generally long lasting as long as you maintain your weight. If you gain weight after liposuction, your fat distribution may change. For example, you may accumulate fat around your abdomen regardless of what areas were originally treated.
|
||
|
|
||
|
|
||
|
What Your Body Does in a Day. This info is unbelievable and incredible to say the least. Sometimes you may feel like your body is beginning to creak and fail you on the outside, but do you ever stop to consider the incredible work that is taking place inside of it? There is so much going on and everything fits together so well, that it's almost impossible to comprehend it.
Click the pic at right, it will remind you that there are miracles going on inside your body every single day. |
||
|
Metabolism and weight loss: How you burn calories.
You've probably heard people blame their weight on a slow metabolism, but what does that mean? Is metabolism really the culprit? And if so, is it possible to rev up your metabolism to burn more calories?
It's true that metabolism is linked to weight. But contrary to common belief, a slow metabolism is rarely the cause of excess weight gain. Although your metabolism influences your body's basic energy needs, how much you eat and drink along with how much physical activity you get are the things that ultimately determine your weight.
Metabolism is the process by which your body converts what you eat and drink into energy. During this complex biochemical process, calories in food and beverages are combined with oxygen to release the energy your body needs to function. Even when you're at rest, your body needs energy for all its "hidden" functions, such as breathing, circulating blood, adjusting hormone levels, and growing and repairing cells. The number of calories your body uses to carry out these basic functions is known as your basal metabolic rate — what you might call metabolism.
Several factors determine your individual basal metabolism, including:
Energy needs for your body's basic functions stay fairly consistent and aren't easily changed. In addition to your basal metabolic rate, two other factors determine how many calories your body burns each day:
Food processing (thermogenesis). Digesting, absorbing, transporting and storing the food you consume also takes calories. About 10 percent of the calories from the carbohydrates and protein you eat are used during the digestion and absorption of the food and nutrients. Physical activity. Physical activity and exercise, such as playing tennis, walking to the store, chasing after the dog and any other movement, account for the rest of the calories your body burns up each day. Physical activity is by far the most variable of the factors that determine how many calories you burn each day.
Scientists call the activity you do all day that isn't deliberate exercise nonexercise activity thermogenesis (NEAT). This activity includes walking from room to room, activities such as gardening and even fidgeting. NEAT accounts for about 100 to 800 calories used daily.
It may be tempting to blame your metabolism for weight gain. But because metabolism is a natural process, your body has many mechanisms that regulate it to meet your individual needs. Only in rare cases do you get excessive weight gain from a medical problem that slows metabolism, such as Cushing's syndrome or having an underactive thyroid gland (hypothyroidism). Unfortunately, weight gain is a complicated process. It's likely a combination of genetic makeup, hormonal controls, diet composition and the impact of environment on your lifestyle, including sleep, physical activity and stress. All of these factors result in an imbalance in the energy equation. You gain weight when you eat more calories than you burn or burn fewer calories than you eat.
While it is true that some people seem to be able to lose weight more quickly and more easily than others, everyone loses weight when they burn up more calories than they eat. To lose weight, you need to create an energy deficit by eating fewer calories or increasing the number of calories you burn through physical activity or both.
While you don't have much control over the speed of your basal metabolism, you can control how many calories you burn through your level of physical activity. The more active you are, the more calories you burn. In fact, some people who are said to have a fast metabolism are probably just more active and maybe fidget more than others.
You can burn more calories with:
Regular aerobic exercise. Aerobic exercise is the most efficient way to burn calories and includes activities such as walking, bicycling and swimming. As a general goal, include at least 30 minutes of physical activity in your daily routine. If you want to lose weight or meet specific fitness goals, you may need to increase the time you spend on physical activity even more. If you can't set aside time for a longer workout, try 10-minute chunks of activity throughout the day. Remember, the more active you are, the greater the benefits. Strength training. Experts recommend strength training exercises, such as weightlifting, at least twice a week. Strength training is important because it helps counteract muscle loss associated with aging. And since muscle tissue burns more calories than fat tissue does, muscle mass is a key factor in weight loss. Lifestyle activities. Any extra movement helps burn calories. Look for ways to walk and move around a few minutes more each day than the day before. Taking the stairs more often and parking farther away from the shops are simple ways to burn more calories. Even activities such as gardening, washing your car and housework burn calories and contribute to weight loss.
Don't look to dietary supplements for help in burning calories or weight loss. Products that claim to speed up your metabolism are often more hype than help, and some may cause undesirable or even dangerous side effects. View these products with caution and scepticism.
There's no easy way to lose weight. The foundation for weight loss continues to be based on physical activity and diet. Take in fewer calories than you burn, and you lose weight.
You know it makes sense!
|
||
|
|
||
|
|
||
|
|
||
|
|
||
|
|
||
|
|