|
|
||
|
||
|
Privacy Policy | Editorial Policy | Profit Policy | Join the Association | List of Members | Contact us | Index | Links |
||
|
Back Go to page: 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Forward
|
||
|
Health and Life Style. |
||
| Veterans and Veterans Families Counselling Service (VVCS) can be reached 24 hours a day across Australia for crisis support and free and confidential counseling. Phone 1800 011 046. VVCS is a service founded by Vietnam Veterans. |
||
|
Fat-free, is it the answer?
For years, leading health organisations have urged us to choose reduced-fat dairy foods, and not too many of them, to protect against heart disease. The accepted wisdom is that reduced fat dairy is lower in saturated fat and helps to maintain healthy cholesterol levels.
But an emerging body of research is questioning the evidence linking saturated fat to cholesterol production and heart disease – the leading cause of death in Australia.
A large study recently published in The Lancet this September adds weight to this body of evidence. It examined data from 130,000 people in 21 countries and found that people who had three servings of full fat dairy foods a day were better off when it came to heart disease risk than those who consumed less than 0.5 servings a day.
Further research published in The American Journal of Clinical Nutrition in July measured the blood levels of three fatty acids found in dairy products of almost 3000 adults aged 65 years and older. The 22-year study found no link between the fatty acids and a higher risk of heart disease or mortality, including fats found in full fat dairy foods.
And an international expert consensus published in the same journal last year reports evidence “does not support a positive association between intake of dairy products and risk of cardiovascular disease”. It said fermented dairy products, such as cheese and yoghurt, were generally associated with improved health outcomes.
The Heart Foundation said research linking full fat dairy foods with a reduced risk of heart disease was inconclusive. It said: “We know there’s different types of saturated fat and they’re found in different types of foods, usually in varying combinations. There is a bit of research into whether saturated fat from dairy has different effects, but there’s nothing conclusive to draw from it at this point in time. Reduced fat dairy is linked to a lower risk of high blood pressure, which is an important risk factor for heart disease, and we don’t see that consistent relationship with full fat dairy.”
It went on to say: “Dairy foods, whether full fat or reduced, did not increase the risk of heart disease”.
The Australian Dietary Guidelines recommend at least two serves of
reduced fat milk, yoghurt and cheese every day. The Heart Foundation
recommends aiming for two to four serves. It said: “Our position is
currently that reduced fat dairy products and unflavoured dairy
products [without added sugar] are the healthier choice. What we
see, time and time again and quite consistently
A professor of clinical and experimental nutrition at the University of Newcastle, said the chemical structure of saturated fat found in dairy foods differed to that found in other foods. This affected the way it was metabolised in the body and its role in disease risk.
“Saturated fat is not a single nutrient, it’s not like vitamin A or vitamin C. We find saturated fat in a variety of foods, like coconut oil, dairy, chocolate, palm oil, eggs and meat. Dairy fat has short chain fatty acids compared to something like palm oil, which has long chain fatty acids.
The way the body metabolises short and medium chain fatty acids is vastly different from the long chain saturated fatty acids.”
It further said: “The scientific community needed evidence that showed a direct, causal relationship between full fat dairy foods and a reduced risk of heart disease. The Lancet study, for example, was observational and therefore unable to show cause and effect. Until that evidence was found, it was unwise to update dietary guidelines. We need to conduct a large intervention trial to show the effects of dairy foods on heart health.
|
||
|
I’ve been to a lot of places but I’ve never been to Cahoots. Apparently you can’t go alone, you have to be in Cahoots with someone. I’ve also never been in Cognito either, I hear no one recognises you there. I have however, been in Sane. They don’t have an airport, you have to be driven there. I have made several trips.
|
||
|
Flu shots.
Every winter in Australia, we hear a horror story or two about someone dying from flu, usually a person who is otherwise fit and healthy, but did you know that influenza actually claims around 3000 deaths each year, is responsible for 18,000 hospitalisations and affects around 350,000 Australians overall? As viruses go, it’s nothing to sniff at — pun intended.
In fact, last year was statistically the worst flu year on record, bringing many ER departments to their knees, and leading the government to invest in a “super flu” shot for Australians over 65. The vaccine has been available in other countries but not here — until now.
All the flu vaccines had been updated for the previous winter and the enhanced vaccines were designed to address the waning immune system that we all have as we age.
|
||
|
|
||
|
Along with the updated quadrivalent influenza vaccines (QIVs), the two types of enhanced flu vaccines available are Fluzone High-Dose, which has four times the amount of active ingredients in the dose and FLUAD, which contains an additional ingredient to boost its effectiveness. It was hoped these vaccines would offer much better protection for older Australians when the flu season hit, particularly against influenza A/H3N2, which experts say is more common and severe in the elderly.
Does a higher dose mean more side effects? A spokesperson for the Royal Australian College of General Practitioners (RACGP), says no. “There is a risk of an increased local reaction, but not of severe adverse reactions’.
They also say that timing is everything. It’s no good heading to your GP to get your shot for next winter as there’s evidence to suggest the effectiveness of the shot might wear off after a few months, so it’s critical you get the vaccine at the right time to ensure you’re covered when peak flu season hits.
“Flu season in Australia is usually June to September, peaking in August, and there’s evidence that the influenza immunisation wears off after three to four months, so it’s important not to have your shots too early.
It takes about three weeks for the vaccine to really kick in and for the immune system to get the full benefit of that vaccine, for that reason, it’s recommended people wait until the end of April, beginning of May, if you’re 65 or older. If you’re younger, having your flu shot around mid-April is probably a good time.
The enhanced vaccines were free for anyone aged 65 and over. Those under 65 had to pay for the revised quadrivalent vaccine, unless they had a certain medical condition. People with chronic heart disease, lung disease, kidney failure, diabetes, or any other chronic illnesses, could be entitled to a free flu shot.
Anyone who’s pooh-poohed the flu shot and come down with influenza knows how brutal it can be. It can really knock you about and it can even be deadly. During the pandemic of 2009, the hospitals where clogged with people in intensive care and we saw that during 2017 season, emergency departments were effectively blocked because of the flu patients. A lot of them end up in ICU, so it can be a very nasty disease.
High risk patients include pregnant women, people over 65, Aboriginal and Torres Strait Islander people, those with complex chronic medical conditions, and kids under five. Kids who are vaccinated actually protect older people, for example, grandparents whose immunity isn’t as strong.
Influenza can come on suddenly and have more severe symptoms than a cold. If you think you have the flu, you need to see your doctor if you develop difficulty breathing, chest pain, sudden dizziness, confusion, severe vomiting, or fever with a rash.
It’s also very important to take time off work and avoid social situations if you have a cold or the flu. Most people are very contagious in the first three to four days of the illness but this can range from one to two days before and last up to five to seven days after the start of symptoms, so it’s important to stay home to not spread the illness. It can take up to two weeks for the symptoms to resolve, and rest and recovery is important.
Next year, if you’re 65 or older, get your shots.
|
||
|
|
||
|
|
||
|
Weight Loss – the right way!
Why do doctors recommend a slow rate of weight loss? What's wrong with fast weight loss?
The concern with fast weight loss is that it usually takes extraordinary efforts in diet and exercise, efforts that could be unhealthy and that you probably can't maintain as permanent lifestyle changes. A weight loss of a half to one Kg a week is the typical recommendation. Although that may seem like a slow pace for weight loss, it's more likely to help you maintain your weight loss for the long term.
Remember that half a Kg of fat contains 3,500 calories, so to lose ½ Kg a week, you need to burn 500 more calories than you eat each day (500 calories x 7 days = 3,500 calories), also, if you lose a lot of weight very quickly, you may not lose as much fat as you would with a more modest rate of weight loss. Instead, you might lose water weight or even lean tissue, since it's hard to burn that many fat calories in a short period.
In some situations, however, faster weight loss can be safe if it's done the right way. For example, doctors might prescribe very low calorie diets for rapid weight loss if obesity is causing serious health problems, but an extreme diet such as this requires medical supervision. In addition, it can be difficult to keep this weight off.
Some diets include an initiation phase to help you jump-start your weight loss. For example, the Mayo Clinic Diet has a quick-start phase in which you might lose 6 to 10 pounds in the first two weeks. You can lose weight quickly with an approach like this because it combines many healthy and safe strategies at once — no gimmicks or extreme dieting.
After the initial two-week period, you transition into the recommended weight loss of one half to one Kg a week, which gives you time to adopt the necessary lifestyle changes, such as eating a healthy diet and increasing your physical activity, necessary for maintaining weight loss over the long term.
But!! Where does the fat go once you lose it??
Isn’t that an interesting question, one day that fat is leading you all around the paddock, you exercise and fast like crazy and soon it’s all gone – but where does it go.
We talk a lot about dieting and burning off fat, but we actually have a lot of misconceptions about weight loss. Some people think fat is converted into energy or heat, a violation of the law of conservation of mass, while others think that the fat is somehow excreted or even converted to muscle. Some people think that you can never lose your fat cells (adipose) once you gain them...they just shrink if you work it off.
Well, none of those are true. According to the University of New south Wales, when you lose weight, you exhale your fat. Its findings, based on existing knowledge about biochemistry, were published in the British Medical Journal recently.
Most of the mass is breathed out as carbon dioxide, It goes into thin air.
Excess carbs and proteins are converted into chemical compounds called triglycerides (which consist of carbon, hydrogen, and oxygen) and then stored in the lipid droplets of fat cells. To lose weight, you’re attempting to metabolize those triglycerides, and that means unlocking the carbon that’s stored in your fat cells.
Losing 10 kilograms of human fat requires the inhalation of 29 kilograms of oxygen, producing 28 kilograms of carbon dioxide and 11 kilograms of water. That’s the metabolic fate of fat. The NSW Uni calculated the proportion of the mass stored in those 10 kilograms of fat that exits as carbon dioxide and as water when we lose weight. By tracing the pathway of those atoms out of the body, it found that 8.4 of those kilograms are exhaled as carbon dioxide. Turns out, our lungs are the primary excretory organ for weight loss. The remaining 1.6 kilograms becomes water, which is excreted in urine, feces, sweat, breath, tears, and other bodily fluids.
So, for this upcoming post-holiday season, should we all just exhale more to shed those extra pounds? No. Breathing more than required by a person’s metabolic rate leads to hyperventilation, followed by dizziness, palpitations, and loss of consciousness.
Check out the video below!
|
||
|
|
||
|
|
||
|
But!!! There’s THIS too
|
||
|
Sugar-less drinks.
Drinking a reasonable amount of diet or sugar-less drinks a day, such as a can or two, isn't likely to hurt you. The artificial sweeteners and other chemicals currently used in these drinks are safe for most people and there's no credible evidence that these ingredients cause cancer. Some types of these drinks are even fortified with vitamins and minerals, but they aren’t a health drink or a silver bullet for weight loss.
Although switching from regular softies to diet or sugar-less softies may save you calories, it's not yet clear if it's effective for preventing obesity and related health problems in the long term. Healthier low-calorie choices abound, including water, skim milk, and unsweetened tea or coffee.
They tell me THIS works too.
|
||
|
Diet tip! If you think you’re hungry, you might just be thirsty. Have a bottle of wine first and then see how you feel.
|
||
|
Womens’ Health.
Breast lump: Early evaluation is essential.
If you find a breast lump or other change in your breast, you might worry about breast cancer. That's understandable, but breast lumps are common and most often they're noncancerous (benign), particularly in younger women. Still, it's important to have any breast lump evaluated by a doctor, especially if it's new, feels different from your other breast or feels different from what you've felt before.
Breasts contain tissues of varying consistency, including fatty, glandular and connective tissue. You might find that breast-related symptoms, such as tenderness or lumpiness, change with your menstrual cycle. Lumps during this time might be caused by extra fluid in your breasts. Breast tissue also changes as you age, typically becoming fattier and less dense.
When to consult your doctor:
Being familiar with how your breasts normally feel makes it easier to detect when there's a change in your breasts. Consult your doctor if:
Evaluation of a breast lump typically begins with a clinical breast exam. During this exam, your doctor will likely:
If your doctor confirms that you have a breast lump or other area of concern, you'll likely need testing.
Procedures to evaluate a breast lump.
Imaging Tests. To further evaluate a breast lump, your doctor might recommend a:
Diagnostic mammogram. This specialized breast X-ray helps your doctor investigate suspicious breast changes. It takes X-ray pictures from several angles.
Breast ultrasound. Sound waves create images of the inside of your breast on a monitor. Ultrasound imaging is helpful for determining whether a breast lump is solid or filled with fluid.
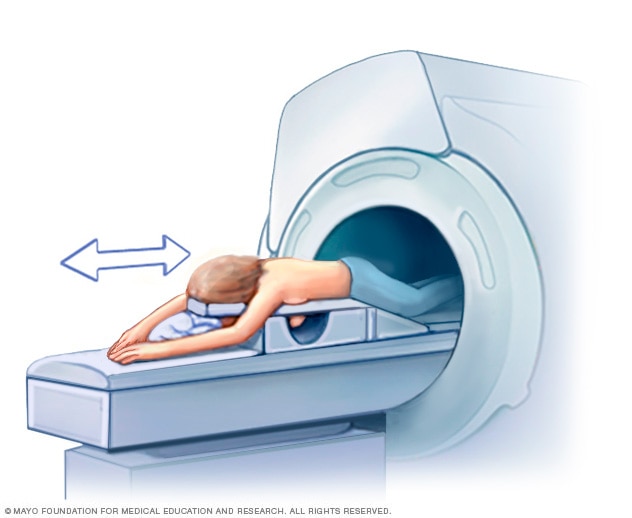
Breast MRI. An MRI machine uses a magnet and radio waves to create pictures of the interior of your breast. During a breast MRI, you lie on your stomach on a padded scanning table. Your breasts fit into a hollow depression in the table, which contains coils that detect magnetic signals. The table slides into the large opening of the MRI machine.
A breast MRI usually is reserved for when the diagnosis is in question. Before a breast MRI, a dye might be injected through an intravenous (IV) line in your arm to enhance the appearance of tissues or blood vessels on the MRI pictures.
Breast biopsy.
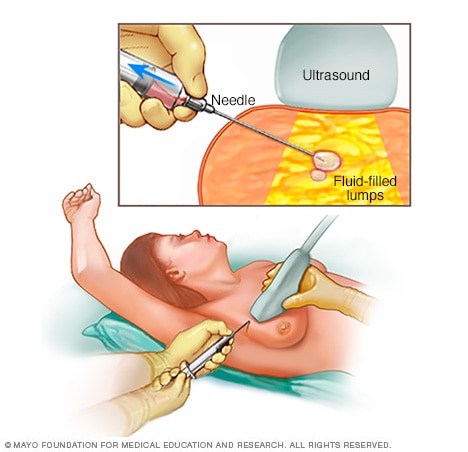
You might have a tissue sample removed and examined under a microscope (biopsy). Ultrasound or mammography might help guide the needle, and a local anaesthetic might be used. Breast biopsy options include:
Fine-needle aspiration biopsy. During fine-needle aspiration, a special needle is inserted into a breast lump and any fluid is removed (aspirated). Ultrasound, a procedure that uses sound waves to create images of your breast on a monitor, might be used to help place the needle.
Core needle biopsy. A core needle biopsy uses a long, hollow tube to extract a sample of tissue. The sample is sent to a laboratory for testing.
Stereotactic biopsy. Mammography produces images of the area in question from several different angles (stereo images). Your doctor then removes a sample of breast tissue with a needle.
Vacuum-assisted biopsy. A probe connected to a vacuum device removes a small sample of breast tissue.
Surgical biopsy. A small cut is made in the skin and breast tissue to remove part or all of a lump.
After a biopsy, the tissue sample is sent to a lab for analysis. Your doctor will let you know when to expect the test results and will discuss them with you when they're available.
Follow-up after breast lump evaluation
If the breast lump isn't cancerous, your doctor will decide if you need short-term monitoring with clinical breast exams or repeat breast imaging. You may be asked to return in two to three months to see if there have been changes in your breast. Consult your doctor if you notice changes in the lump or develop new areas of concern.
If the diagnosis is in question, the clinical breast exam and the mammogram show areas of suspicion, for example, but the biopsy reveals benign tissue, you'll be referred to a surgeon or other specialist for further consultation.
If the breast lump is cancerous, you'll work with your doctor to create a treatment plan. The stage and type of breast cancer will influence your treatment options.
|
||
|
|
||
|
|
||
|
Grapefruit juice.
I like to drink grapefruit juice but hear that it can interfere with some prescription medications. Is that true?
Yes! Grapefruit and certain other citrus fruits, such as bitter or sour oranges (a cross between a pomelo and a mandarin), can interfere with several kinds of prescription medications. Don't take these interactions lightly. Some can cause potentially dangerous health problems. If you take prescription medication, ask your doctor or pharmacist whether your medication interacts with grapefruit or other citrus products.
You may need to eliminate grapefruit products from your diet. Simply taking your medication and grapefruit product at different times doesn't stop the interaction. Alternatively, you can ask your doctor if there's a comparable medication you can take that doesn't interact with grapefruit.
Problems arise because chemicals in the fruit can interfere with the enzymes that break down (metabolize) the medication in your digestive system. As a result, the medication may stay in your body for too short or too long a time. A medication that's broken down too quickly won't have time to work. On the other hand, a medication that stays in the body too long may build up to potentially dangerous levels.
The list of medications that can interact with grapefruit includes
commonly prescribed medications that:
Another potential problem is that some foods and drinks may contain grapefruit but don't say so in the name or on the ingredients list. For example, numerous citrus-flavoured soft drinks contain grapefruit juice or grapefruit extract.
Play it safe with prescription drugs. Always ask your doctor or pharmacist when you get a new prescription if it interacts with any foods or other medicines. If the answer is yes, ask whether you need to eliminate that food from your diet.
|
||
|
|
||
|
|
||
|
|
||
|
|
||
|
|
||
|
|
||
|
|